Relationship Between Physiological Umbilical Herniation and Liver Morphogenesis During the Human Embryonic Period: A Morphological and Morphometric Study
ヒト胚子期に形成される一次腸ループは、臍帯内の胚外体腔中へ一時的に脱出後(生理的臍帯ヘルニア[Physiological umbilical herni; PUH] )、胎児期初期に腹腔内へ還納する。PUHの原因は、同時期に肝臓が急速に成長して腹腔の多くを占める結果、腹腔が一過性に一次腸ループを入れるには足りないため、と1899年に報告されてから詳細な解析は行われていない。2018年に報告した肝臓形成異常群の中から(Kanahashi et al)、Carnegie stage (CS)21の肝臓低形成、無形成4例にPUHが確認された。PUHの発生要因をさらに検討するため、上記4例と正常2例を用いて肝臓の形態形成との関連に基づいた詳細な形態観察と形態計測による解析を行った。肝臓無形成1例(AG1)を除く3例は、盲腸が正常例と同様に上腸間膜動脈の左側に位置していたが、AG1は腸ループの先端に位置していた。腸ループの遠位端にあたる胚外体腔と腹腔の境界部分は正常例とAG1では腸管が直線的にみられたが、残り3例は境界部分に二次腸ループがみられた。上部消化管(胃、十二指腸)と膵臓は4例全てで胃の噴門部と、膵臓・十二指腸の接合部の2点が正常例とほぼ同じ位置を示したが、その他の部位に偏位がみられた。肝臓低形成・無形成4例と正常例では、腸ループの長さや腸ループが胚外体腔へ出ている割合はほぼ同じであった。4例の腹腔体積値は正常例と比較して明らかに小さかったが、腹腔内の腸管体積推定値は正常例とほぼ同等であった。PUHは中腸と腹腔スペースの両者がほぼ正常に成長することによって引き起こされ、腸管の成長やPUHの発生は肝臓の成長とは無関係であることが示唆された。
Kanahashi T, Yamada S, Yoneyama A, Takakuwa T. Relationship Between Physiological Umbilical Herniation and Liver Morphogenesis During the Human Embryonic Period: A Morphological and Morphometric Study. Anat Rec 2019, 302, 1968-1976. doi: 10.1002/ar.24149.
Kanahashi T, Yamada S, Tanaka M, Hirose A, Uwabe C, Kose K, Yoneyama A, Takeda T, Takakuwa T, A novel strategy to reveal the latent abnormalities in human embryonic stages from a large embryo collection, Anatomical Record, 299,8-24,2016 10.1002/ar.23281(概要), *299(1),2016の表紙に採用されました。DOI: 10.1002/ar.23206 (cover page)
40. Matsubayashi J, Okuno K, Fuji S, Ishizu K, Yamada S, Yoneyama A, Takakuwa T. Human embryonic ribs all progress through common morphological forms irrespective of their position on the axis, Dev Dyn 2019, 248, 1257-1263, doi: 10.1002/dvdy.107
parsimonious model
Abstract
Background
We aimed to analyze the morphogenesis of all ribs from 1st to 12th rib pairs plus vertebrae to compare their differences and features according to the position along the cranial-caudal axis during the human embryonic period.
Results
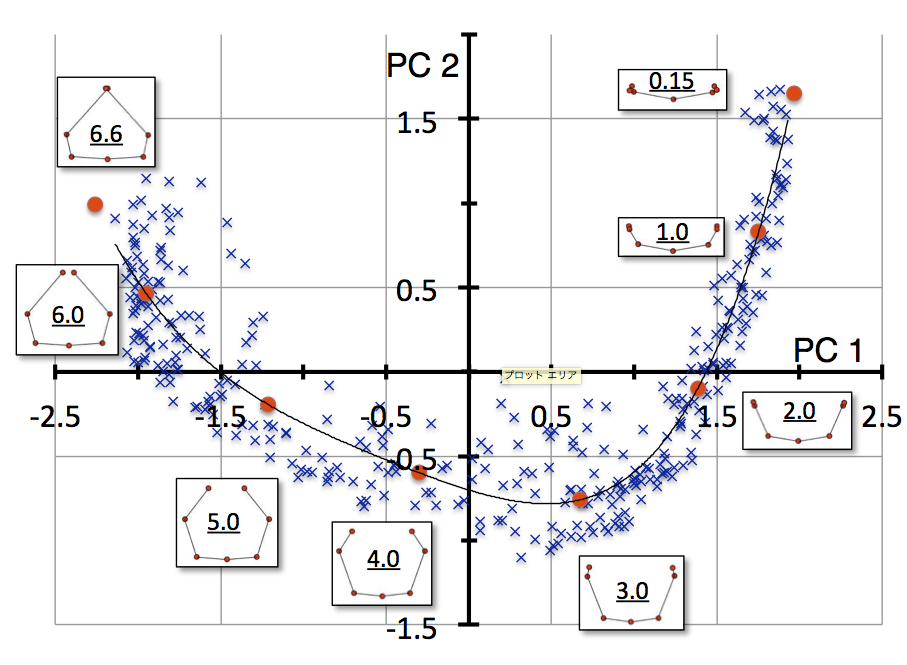
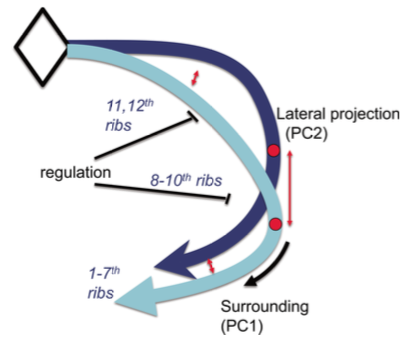
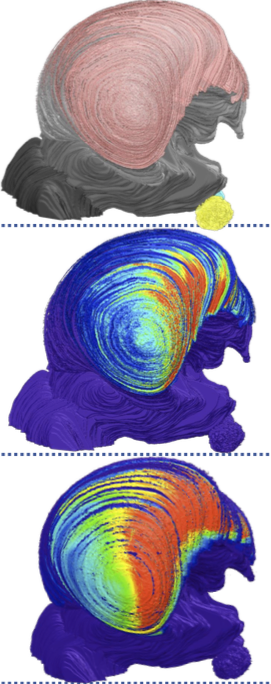
Rib pair formation was analyzed using high-resolution digitalized imaging data (n = 29) between Carnegie stage (CS) 18 and CS23 (corresponding to ED13-14 in mouse; HH29-35 in chick). A total of 348 rib pairs, from 1st to 12th rib pairs of each sample were subjected to Procrustes and principal component (PC) analyses. PC1 and PC2 accounted for 76.3% and 16.4% (total 92.7%) of the total variance, respectively, indicating that two components mainly accounted for the change in shape. The distribution of PC1 and PC2 values for each rib showed a “fishhook-like shape” upon fitting to a quartic equation. PC1 and PC2 value position for each rib pair moved along the fitted curve according to the development. Thus, the change in PC1 and PC2 could be expressed by a single parameter using a fitted curve as a linear scale for shape.
Conclusion
Human embryonic ribs all progress through common morphological forms irrespective of their position on the axis.
Okuno K, Ishizu K, Matsubayashi J, Fujii S, Sakamoto R, Ishikawa A, Yamada S, Yoneyama A, Takakuwa T. Rib cage morphogenesis in the human embryo: A detailed three-dimensional analysis. Anat Rec 2019, 302, 2211-2223, doi: 10.1002/ar.24226
ABSTRACT
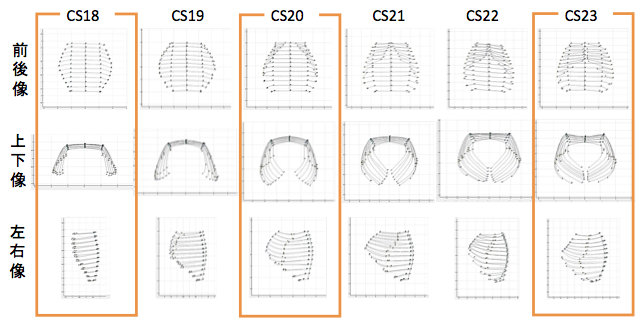
Formation of the skeletal structure in the human embryo has important consequences in terms of support, protection, and function of organs and other systems. We aimed to describe the formation of the rib cage during the embryonic period, in order to detect prominent features and identify the possible factors affecting rib cage morphology. We employed high-resolution digitized imaging data (n = 34) obtained in human embryos with Carnegie stage (CS) between 17 and 23. The rib cage became detectable as cartilage formation at CS17, expanding outward from the dorsal side of the chest-abdominal region. Ribs elongated progressively to surround the chest, differentiating into the upper and lower rib cage regions by CS20. The ends of corresponding ribs in the upper region elongated toward each other, leading to their joining and sternum formation between CS21 and CS23, while the lower region of the rib cage remained widely open. The rib cage area with the largest width shifted from the 5th rib pair at CS17 to the 9th pair at CS23. The depth of the rib cage was similar across the upper region at CS17, with the major portion remaining in the middle part after CS20. The heart was located beneath the rib pairs providing the largest depth, while the liver was located beneath the rib pairs providing the largest width. Formation of the sternum, development of spinal kyphosis, and organization of larger internal organs within the thoracic and abdominal cavity are possible factors affecting rib cage morphology. Anat Rec, 302:2211–2223, 2019.
37. Ishiyama H, Ishikawa A, Imai H, Matsuda T, Yoneyama A, Yamada S, Takakuwa T. Spatial relationship between the metanephros and adjacent organs according to the Carnegie stage of development. Anat Rec 2019. 302, 1887-2104. DOI: 10.1002/ar.24103
ABSTRACT
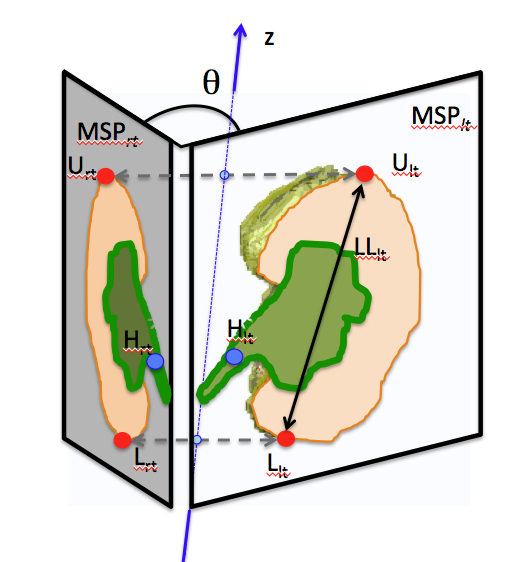
The morphological changes in the metanephros and its spatial relationship to the adjacent organs was evaluated based on the Carnegie stages (CSs) from 14 through 23. The imaging modalities used included magnetic resonance imaging (N = 4), phase-contrast X-ray computed tomography (N = 11), and serial histological sections (N = 40), supplemented by three-dimensional image reconstruction. The orientation of the hilus of the metanephros changed significantly between CS17 (34.4 ± 13.7 degrees) and 18 (122.3 ± 38.1 degrees), with an increase in the number of branches of the urinary collecting system, from 1.61 ± 0.42 at CS17 to 3.20 ± 0.35 at CS18. This increase in the number of branches influenced the growth of the metanephros and the orientation of its hilus. The right and left metanephroses were in proximity throughout the embryonic period. The local maximum interpole distances were observed at CS18 (0.87 ± 0.11 mm for the upper and 0.50 ± 0.25 mm for the lower pole). Mesenchymal tissue was observed between the metanephros and iliac arteries, as well as between the right and left metanephros. Throughout development, the position of the lower pole of the metanephros remained adjacent to the aortic bifurcation. The position of the upper pole, referenced with respect to the aortic bifurcation, increased by >2.0 mm, reflecting the longitudinal growth of the metanephros. Our findings provide a detailed description of the morphogenesis of the metanephros and of its hilus, which might contribute to our understanding of congenital malformations and malpositions of the kidneys.
Kanahashi T, Yamada S, Yoneyama A, Takakuwa T. Relationship Between Physiological Umbilical Herniation and Liver Morphogenesis During the Human Embryonic Period: A Morphological and Morphometric Study. Anat Rec 2019, 302, 1968-1976. doi: 10.1002/ar.24149.
肝臓無形成でも生理的臍帯ヘルニアがみられる
ABSTRACT
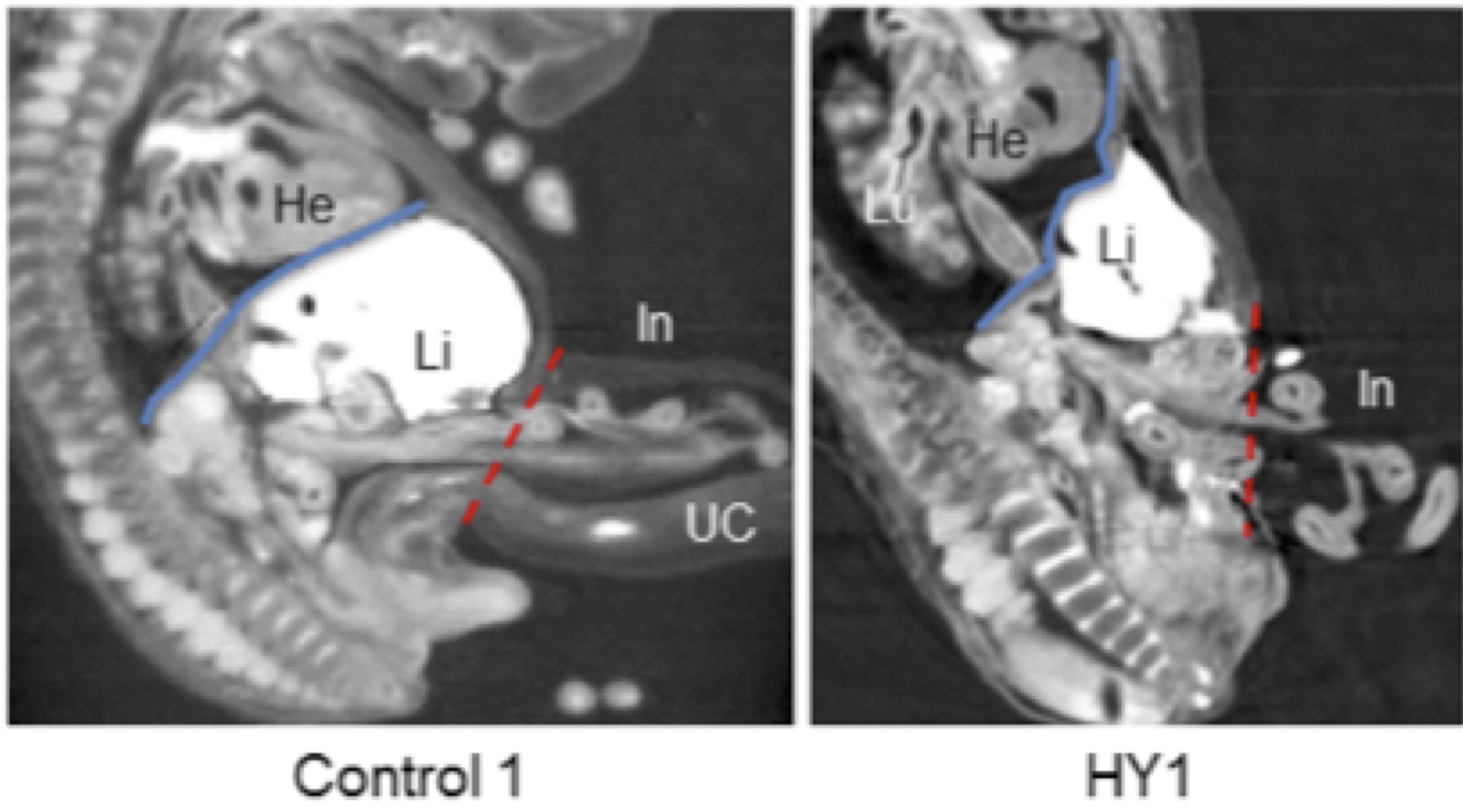
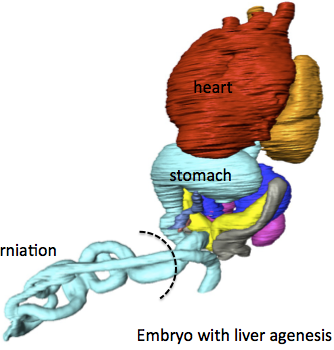
It is widely hypothesized that physiological umbilical herniation (PUH) in humans occurs, because the liver occupies a large space in the abdominal cavity, which pushes the intestine into the extraembryonic coelom during the embryonic period. We have recently shown the presence of the intestinal loop in the extraembryonic coelom in embryos with liver malformation. Here, we analyzed the relationship between the liver and the PUH at Carnegie stage 21 of four embryos with liver malformation, including two with hypogenesis (HY1, HY2) and two with agenesis (AG1, AG2), using phase-contrast X-ray computed tomography and compared them with two control embryos. The intestinal loop morphology in the malformed embryos differed from that in the control embryos, except in HY1. The length of the digestive tract in the extraembryonic coelom of the embryos with liver malformation was similar to or longer than that of the controls. The rate of intestinal loop lengthening in the extraembryonic coelom compared with that of the total digestive tract in all embryos with liver malformation was similar to or higher than that of the controls. The estimated total abdominal cavity volume in the embryos with liver malformation was considerably smaller than that of the controls, while the intestinal volume was similar. The cardia and proximal portion of the pancreas connecting to the duodenum were located at almost identical positions in all the embryos, whereas other parts of the upper digestive tract deviated in the embryos with abnormal livers. Thus, our results provided evidence that PUH occurred independently of liver volume.
Suzuki Y, Matsubayashi J, Ji X, Yamada S, Yoneyama A, Imai H, Matsuda T, Aoyama T, Takakuwa T Morphogenesis of the femur at different stages of normal human development, PLoS ONE, 14(8): e0221569. https://doi.org/10.1371/journal. pone.0221569
Abstract
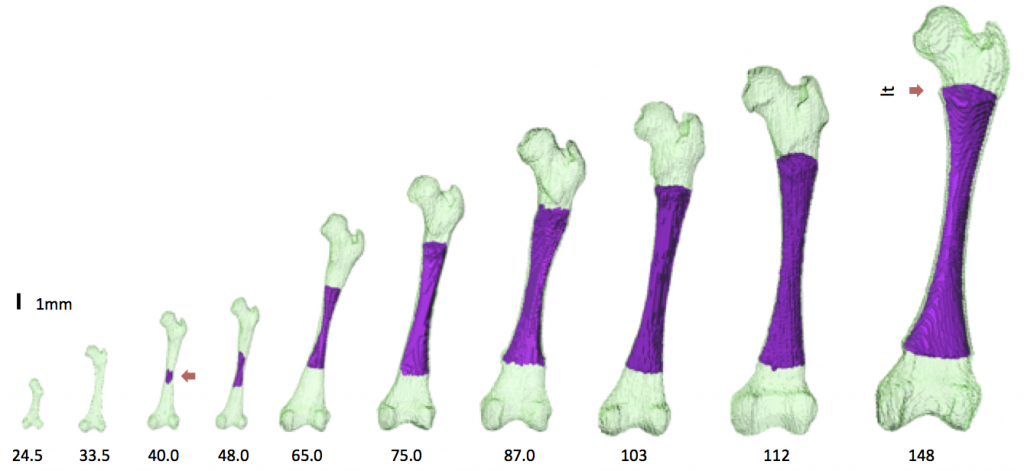
The present study aimed to better characterize the morphogenesis of the femur from the embryonic to the early fetal periods. Sixty-two human fetal specimens (crown–rump length [CRL] range: 11.4–185 mm) from the Kyoto Collection were used for this study. The morphogenesis and internal differentiation process of the femur were analyzed in 3D using phase-contrast X-ray computed tomography and magnetic resonance imaging. The cartilaginous femur was first observed at Carnegie stage 18. Major anatomical landmarks were formed prior to the initiation of ossification at the center of the diaphysis (CRL, 40 mm), as described by Bardeen. The region with very high signal intensity (phase 5 according to Streeter’s classification; i.e., area described as cartilage disintegration) emerged at the center of the diaphysis, which split the region with slightly low signal intensity (phase 4; i.e., cartilage cells of maximum size) in fetuses with a CRL of 40.0 mm. The phase 4 and phase 5 regions became confined to the metaphysis, which might become the epiphyseal cartilage plate. Femur length and ossified shaft length (OSL) showed a strong positive correlation with CRL. The OSL-to-femur length ratio rapidly increased in fetuses with CRL between 40 and 75 mm, which became moderately increased in fetuses with a CRL of ≥75 mm. Cartilage canal invasion occurred earlier at the proximal epiphysis (CRL, 62 mm) than at the distal epiphysis (CRL, 75 mm). Morphometry and Procrustes analysis indicated that changes in the femur shape after ossification were limited, which were mainly detected at the time of initial ossification and shortly after that. In contrast, femoral neck anteversion and torsion of the femoral head continuously changed during the fetal period. Our data could aid in understanding the morphogenesis of the femur and in differentiating normal and abnormal development during the early fetal period.







 金橋くんの博士審査会が行われました。(1/16(木)10:30- 高井ホール)
金橋くんの博士審査会が行われました。(1/16(木)10:30- 高井ホール)