






長田さん、八田くんの卒業論文がJournal of Anatomy に掲載されました。
ヒトの消化管は一時的に臍帯内に脱出しCRL40 mmころ、突然還納します(生理的ヘルニア)。生理的ヘルニアの脱出については論文がある程度ありますが、還納過程については研究がほとんどなく、不明な点が多くありました。今回の解析では、還納途中の3体を含む25体について形態計測的な検討をし以下の知見をえました。
- 腹腔内での占拠割合は徐々に消化管が上昇、肝臓が減少し急激な変化はみられない
- 消化管還納終了時、腹腔内で使用可能な消化管体積は200mm3で、臍帯内の最大容積25.8mmに比べ十分に大きい
- ヘルニア期の腸管の最大の高さよりも、還納後の腹壁(臍帯輪)の高さは高い
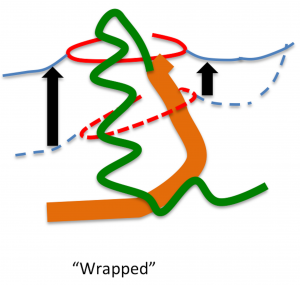
- 消化管還納時には、腹腔内へ張力が働く(loop model)という古典的な説に対して、
- 腹壁がもちあがり消化管を包むことが起きている可能性を提唱(wrapping model)
35. Nagata A, Hatta S, Ji X, Ishikawa A, Sakamoto R, Yamada S, Imai H, Matsuda T, Takakuwa T. Return of the intestinal loop to the abdominal coelom after physiological umbilical herniation in the early fetal period. J Anat, 2019, 234, 456-464.doi: 10.1111/joa.12940.
Abstract
The intestine elongates during the early fetal period, herniates into the extraembryonic coelom, and subsequently returns to the abdominal coelom. The manner of herniation is well-known; however, the process by which the intestinal loop returns to the abdomen is not clear. Thus, the present study was designed to document and measure intestinal movements in the early fetal period in three dimensions to elucidate the intestinal loop return process. Magnetic resonance images from human fetuses whose intestinal loops herniated (herniated phase; n = 5) while returning to the abdominal coelom [transition phase; n = 3, crown–rump length (CRL)] 37, 41, and 43 mm] and those whose intestinal loops returned to the abdominal coelom normally (return phase; n = 12) were selected from the Kyoto Collection. Intestinal return began from proximal to distal in samples with CRL of 37 mm. Only the ileum ends were observed in the extraembryonic coelom in samples with CRLs of 41 and 43 mm, whereas the ceca were already located in the abdominal coeloms. The entire intestinal tract had returned to the abdominal coelom in samples with CRL > 43 mm. The intestinal length increased almost linearly with fetal growth irrespective of the phase (R2 = 0.90). The ratio of the intestinal length in the extraembryonic coelom to the entire intestinal length was maximal in samples with CRLs of 32 mm (77%). This ratio rapidly decreased in three of the samples that were in the transition phase. The abdominal volumes increased exponentially (to the third power) during development. The intestinal volumes accounted for 33–41% of the abdominal volumes among samples in the herniated phase. The proportion of the intestine in the abdominal cavity increased, whereas that in the liver decreased, both without any break or plateau. The amount of space available for the intestine by the end of the transition phase was approximately 200 mm3. The amount of space available for the intestine in the abdominal coelom appeared to be sufficient at the beginning of the return phase in samples with CRLs of approximately 43 mm compared with the maximum intestinal volume available for the extraembryonic coelom in the herniated phase, which was 25.8 mm3 in samples with CRLs of 32 mm. A rapid increase in the space available for the intestine in the abdominal coelom that exceeded the intestinal volume in the extraembryonic coelom generated an inward force, leading to a ‘sucked back’ mechanism acting as the driving force. The height of the hernia tip increased to 8.9 mm at a maximum fetal CRL of 37 mm. The height of the umbilical ring increased in a stepwise manner between the transition and return phases and its height in the return phase was comparable to or higher than that of the hernia tip during the herniation phase. We surmised that the space was generated in the aforementioned manner to accommodate the herniated portion of the intestine, much like the intestine wrapping into the abdominal coelom as the height of the umbilical ring increased.